Published March 2024
Overview of logic model
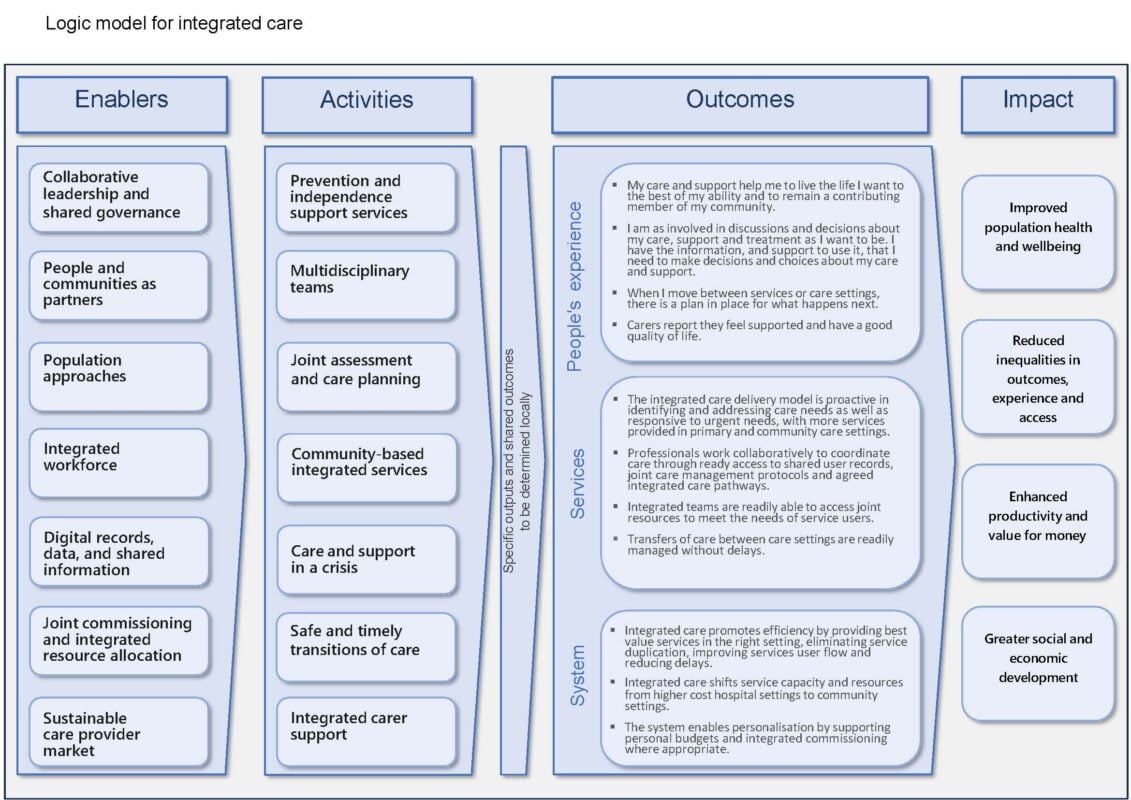
The logic model for integrated care describes what good looks like, providing a visual depiction of how a fully integrated health and care system might be structured and function, and the outcomes and benefits it should deliver for those who use services and their carers. It describes:
- the enablers of integration
- the key activities of integrated care
- the outcomes for people who use services, for the integrated services and for the wider health and care system
- the long-term impacts and benefits.
Enablers
Activities
Outcomes
Impact
Stakeholders who contributed to developing the logic model suggested it would be a useful tool for local planning and performance monitoring. We encourage you to use the logic model for this purpose, and to provide us with your feedback.
Download the logic model (enablers, activities, outcomes and impact)
This image provides the overall structure of the logic model and gives a visual representation of how the different elements of the logic model (enablers and activities) connect.
The enablers and activities are set out underneath in more detail.
Enablers and activities
The contextual factors that create the pre-conditions for integrated care.
The types of interventions and services that create integration, and the primary settings where integration occurs.
Systems
- Integrated care promotes efficiency by providing best value services in the right setting, eliminating service duplication, improving services user flow and reducing delays.
- Integrated care shifts service capacity and resources from higher cost hospital settings to community settings.
- The system enables personalisation by supporting personal budgets and integrated commissioning where appropriate.
Services
- The integrated care delivery model is proactive in identifying and addressing care needs as well as responsive to urgent needs, with more services provided in primary and community care settings.
- Professionals work collaboratively to coordinate care through ready access to shared user records, joint care management protocols and agreed integrated care pathways.
- Integrated teams are readily able to access joint resources to meet the needs of service users.
- Transfers of care between care settings are readily managed without delays.
People's experiences
- My care and support help me to live the life I want to the best of my ability and to remain a contributing member of my community.
- I am as involved in discussions and decisions about my care, support and treatment as I want to be. I have the information, and support to use it, that I need to make decisions and choices about my care and support.
- When I move between services or care settings, there is a plan in place for what happens next.
- Carers report they feel supported and have a good quality of life.